News & Updates

Authors: DeAngelis AF, Barrowman RA, Harrod R, Nastri AL
Abstract
Dentoalveolar trauma and dislocations of the temporomandibular joint are common reasons for patients to present to EDs in Australia. The majority of medical practitioners receive very little formal training in the management of these injuries and might not have ready access to dental services out of hours for advice. This article focuses on the emergency assessment, triage and non-specialist management of dentoalveolar trauma and injuries to the temporomandibular joint.
Chow SP1, Nastri A, Hardy T.
Abstract
Inflammatory myofibroblastic tumour (IMT) is a rare distinctive neoplasm of intermediate biological potential with a predilection for the abdominopelvic region and lung of children and young adults. It is histologically composed of spindle cells (myofibroblasts) in a myxoid to collagenous stroma with a prominent inflammatory infiltrate composed primarily of plasma cells and lymphocytes. Its pathogenesis is controversial.
Arising most commonly in the lungs, only two cases of histopathologically confirmed IMT originating from the infratemporal and pterygopalatine fossae have been documented in the literature. Neither had orbital involvement. We now report the first case of IMT originating from the infratemporal fossa with orbital extension in a previously well 31-year-old woman. The patient presented with a 5-month history of intermittent right-sided headaches, progressive trismus and right lower lid swelling. She then developed right proptosis, diplopia and paraesthesia in the ophthalmic and maxillary divisions of her trigeminal nerve.
Magnetic resonance imaging showed a soft tissue mass occupying most of the right infratemporal fossa with extension into pterygopalatine fossa and orbit. Provisional diagnosis from an open biopsy was nodular fasciitis. She underwent surgical debulking of the infratemporal fossa and lateral orbit through a coronal and trans-oral approach with trans-zygomatic access via total zygomatic osteotomy. Review of intraoperative specimens revised the diagnosis to IMT. Further management included systemic corticosteroids and adjuvant radiotherapy.
Authors: DeAngelis AF, Barrowman RA, Harrod R, Nastri AL.
Abstract
Oral pain and odontogenic infections are common reasons for patients to present to EDs and general medical practice in Australia. Although most odontogenic infections can be managed on an outpatient basis, because of their proximity to the airway, infections in this region can be life-threatening, requiring urgent surgical intervention and ICU management. This article focuses on the emergency assessment, triage and non-specialist management of oral pain and odontogenic infections.
A lot of people don’t have enough space for wisdom teeth when they erupt, and as a result, experience pain, as well as tooth decay and other oral health issues. But what are impacted wisdom teeth, exactly? And, what can you expect from a removal procedure?
What are impacted wisdom teeth?
In most cases, wisdom teeth become impacted when there is not enough space for the teeth in the jaw. Wisdom teeth can also grow at an angle, causing them to become impacted. This can cause pain and discomfort, as well as a number of other issues, including tooth decay and damage to the surrounding teeth and gums.
What are the symptoms?
While some people won’t have any issues, others will experience some very clear signs that their wisdom teeth are impacted. Some of the most common symptoms include very intense pain in the mouth. In fact, this pain may even extend to the ear and throat and can cause considerable discomfort. Impacted wisdom teeth can also cause swelling in the face, as well as in the gum line at the back of the mouth. If a tooth becomes infected, one may notice an unusual (and unpleasant) taste in the mouth, bad breath, and difficulty opening the mouth, as well as bleeding gums and pain in the jaw.
Is it necessary to remove wisdom teeth?
It’s not always necessary to remove wisdom teeth — some people have enough space for their teeth to erupt without surgical intervention. For others, however, there is simply not enough space in the jaw for wisdom teeth to erupt without having an effect on the surrounding teeth and gums. We recommend removing wisdom teeth if there is infection, disease, cysts or tumours around the teeth. If you experience any uncomfortable and painful symptoms, you are likely to benefit from a removal procedure.
If you’re concerned about the implications of having your wisdom teeth removed, bear in mind that wisdom teeth are actually not necessary for our modern diets and lifestyles. They are an evolutionary remnant that are no longer essential to our survival, so you don’t have to worry about life without them. In fact, if your wisdom teeth have become impacted and are causing crowding in your mouth, they can do more harm than good and lead to a range of health issues.
What does the wisdom tooth removal procedure involve?
Before the surgery, we will examine your teeth and mouth to confirm that your wisdom teeth have become impacted and that a removal procedure is the best treatment option for you. We’ll take an x-ray to assess any damage of the surrounding teeth and bones.
You’ll be given an anaesthetic before we make a small incision in your gums. Any problematic bone will be removed along with the wisdom teeth. Depending on the case, the teeth may be removed in pieces. The incision will be carefully closed with stitches, and your wound will be dressed in gauze. The entire procedure generally only takes between 30 and 60 minutes to complete.
It’s quite normal to experience some swelling and pain after surgery, so we recommend that you stick to soft foods for around a week following the procedure. Try foods like soups, mashed potatoes, yoghurt and ice cream to minimise chewing.
Have you noticed any discomfort, pain or swelling around the back of your mouth? It’s possible that you might require wisdom tooth surgery. Get in touch with us to make an appointment and we’ll perform a thorough examination before recommending a treatment plan.
Abstract
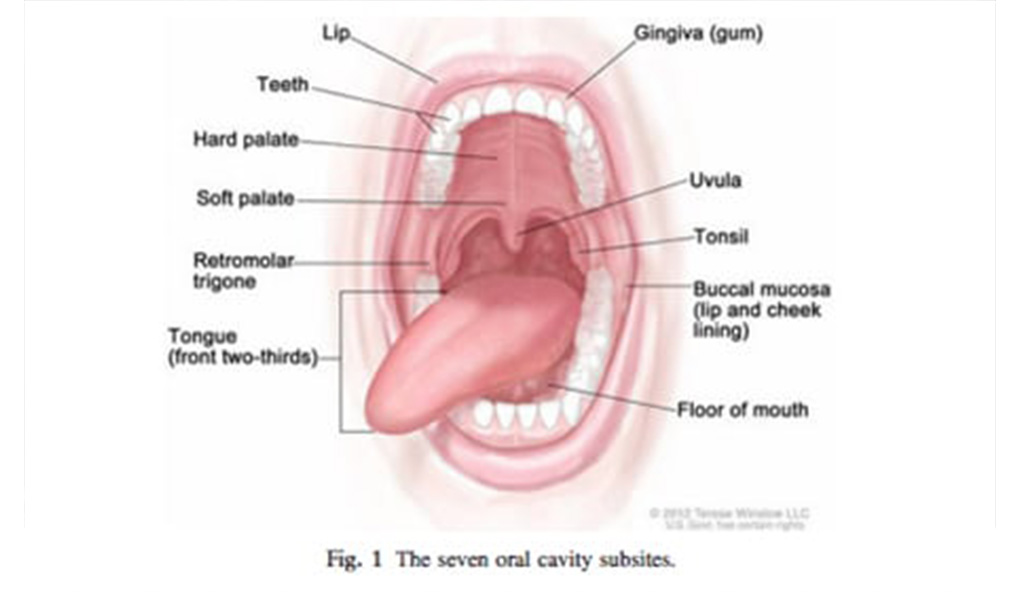
The management of oral cancer is a multidisciplinary endeavour, as each patient presents the treating clinicians with a unique set of challenges the management of which impacts on both survival and quality of life. This article focuses on the management of oral cancer. We highlight the epidemiology and risk factors for oral cancer in Australia, the various clinical presentations that occur and the staging of oral cancer. In the vast majority of cases surgery remains the mainstay of treatment. Radiation and medical oncology is usually used in an adjuvant context. Dental professionals play a critical role in many stages of management from the initial detection, to optimising pre treatment dental health and managing the short and long term sequelae of treatment. Monitoring for recurrence and the development of second primary tumours is a key role.
L Kaing,* S Manchella,* C Love,* A Nastri,*† D Wiesenfeld*†
*The Royal Melbourne Hospital, Melbourne, Victoria, Australia. †Department of Surgery and Melbourne Dental School, The University of Melbourne, Victoria, Australia.
Abstract
Background: The aim of this study was to identify changes in referral patterns and delays in diagnosis and treatment of oral squamous cell carcinoma (OSCC), managed at a tertiary institution in Victoria, Australia. Methods: The hospital records of all patients with newly diagnosed OSCC, managed by The Royal Melbourne Hospital (RMH) Head and Neck Tumour Stream between January 2008 and December 2010, were retrospectively reviewed.
Results: Of the 101 patients, 52% first sought help from general medical practitioners (GMP) while 43% initially attended a general dental practitioner (GDP). The most common site of OSCC was oral tongue (42%). The most common presentation was ulceration (31%). Seventy per cent of patients presented with T1 (39%) or T2 (31%) tumours. The diagnostic delay ranged from 0 to 8 years with an average of 4.5 months. Patient delay ranged from 0 to 1.4 years with an average of 1.8 months. Professional delay ranged from 0 to 8 years with an average of 2 months.
Conclusions: Delays in patients seeking advice have decreased compared to previous studies, while delays in professionals making a diagnosis have not improved considerably. There has been a significant shift towards initial presentation to GMP rather than GDP. Further decrease in delays is possible by improving both population awareness and clinician education.
Abstract
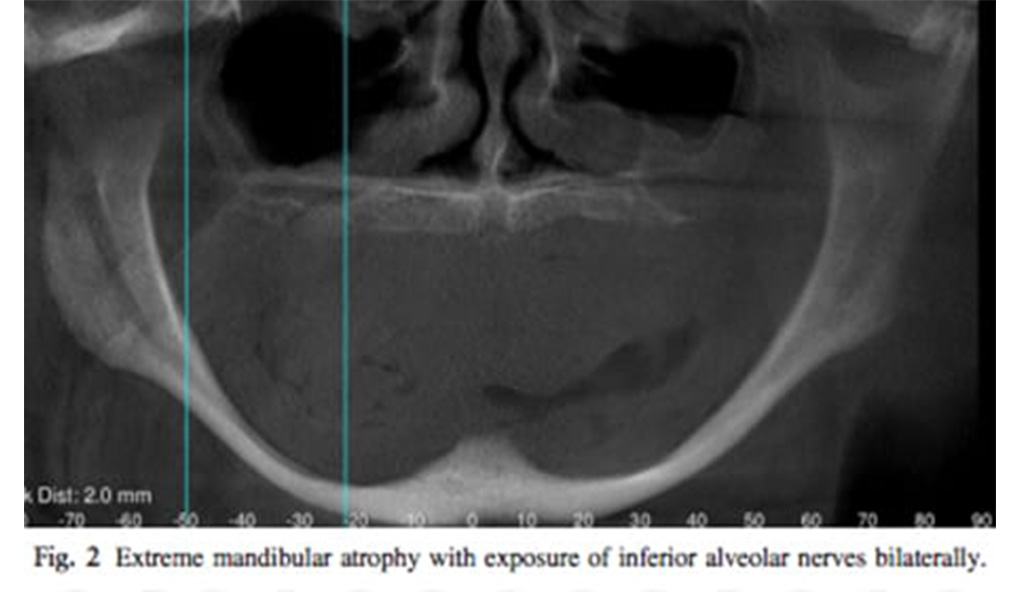
The atrophic and edentulous jaw can pose a number of challenges for the implant clinician. In simple terms, the amount of bone that remains is insufficient for the conventional placement of a dental implant. A variety of treatment strategies can be employed to enable implants to be placed despite the paucity of bone stock in either the mandible or the maxilla. Conceptually these strategies follow one of two pathways: either augmentation of the bone, or the novel utilization of the remaining bone. This article will discuss patient assessment, treatment planning, and the range of contemporary options available to enable fixed implant based rehabilitation of each jaw. “The edentulous patient is an amputee, an oral invalid, to whom we should pay total respect and rehabilitation ambitions” (P-I Branemark, September 2005).
Abstract
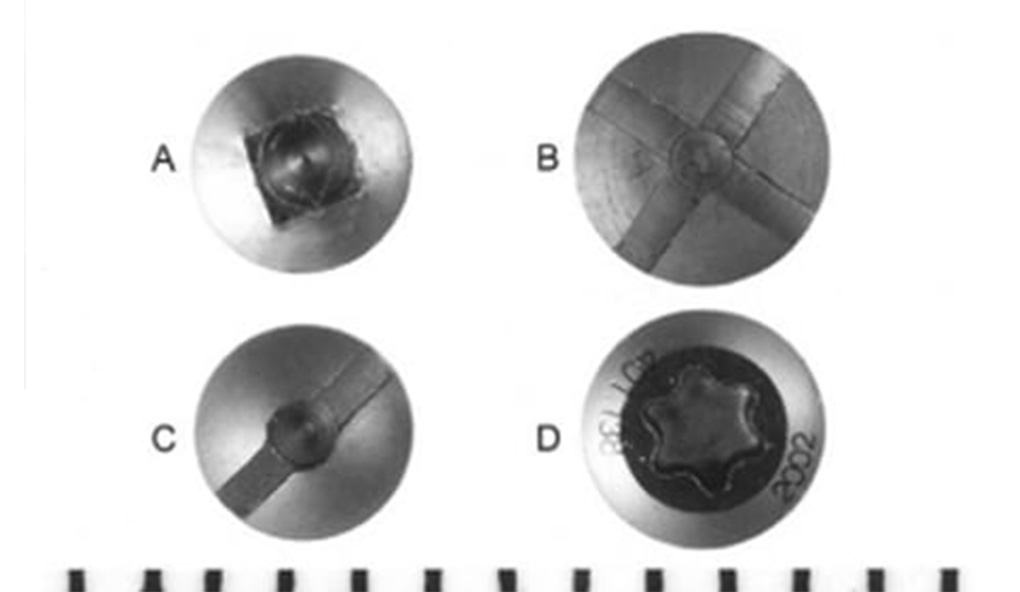
Purpose: This experimental study was designed to examine whether screw head design influenced the angle of application of a screwdriver at which failure of engagement or stripping of the screw head occurred.
Materials and Methods: Four different screw head designs (slot, cross, square, star) were tested in a custom-made jig that was designed to enable the screws to be tested over a range of angles of application of the respective screwdrivers, to determine whether the screw head design influenced the torque value at which the screw head stripped or failure of driver engagement occurred.
Results: The results fell clearly into 2 groups: The slot and cross designs gave the highest torque values at all angles, while the torque values for the square and star designs dropped to a low value with increasing angulation between the screw and driver. These differences were significant (P < .001).
Conclusions: Although this experimental situation cannot be entirely extrapolated to the clinical situation, it indicates that the slot or cross design may offer an advantage in regions of difficult access where the angulation of the screwdriver to the screw may of necessity be increased.
© 2004 American Association of Oral and Maxillofacial Surgeons J Oral Maxillofac Surg 62:473-478, 2004.
Abstract
Purpose of review
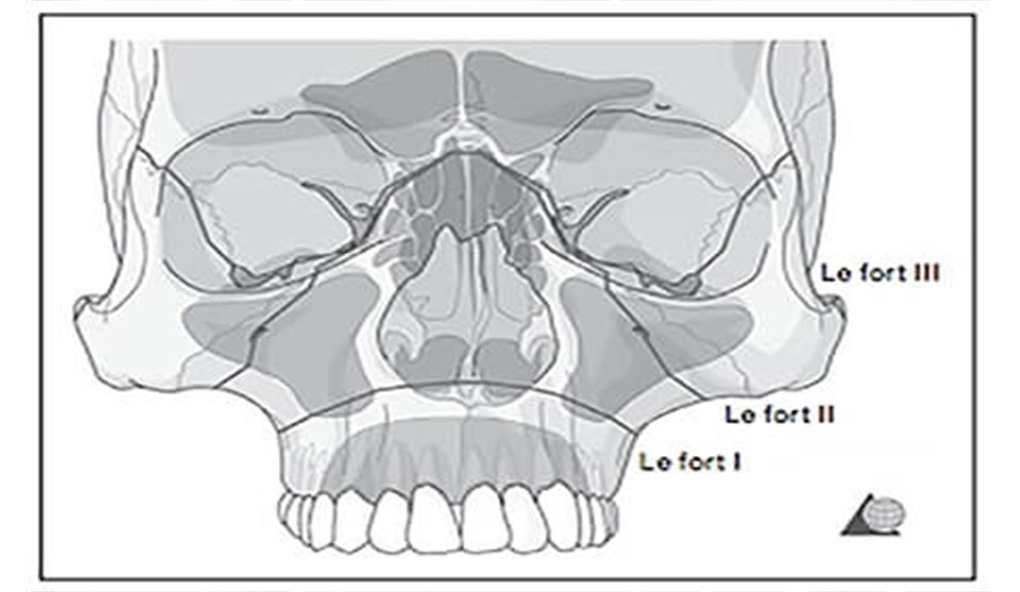
Management of midface trauma is complex and challenging and requires a clear understanding of the facial buttress system, subunit anatomy and inter-relationships. Too often clinicians attempt surgical repair without adequate knowledge of the common complications associated with poor reduction and improper sequencing of fracture repair. This review outlines a working approach to the identification and management of such injuries, and the definitive management of common injury patterns.
Recent findings
Midface trauma, with or without life-threatening and sight-threatening complications, may arise following isolated injury, or be associated with significant injuries elsewhere. Assessment needs to be both systematic and repeated, with the establishment of clearly stated priorities in overall care.
Summary
Accurate and precise relocation of bony subunits and resuspension of soft tissues is vital in achieving acceptable functional and aesthetic outcomes.
Keywords
facial buttress, Le Fort, midface fracture, zygomatico-maxillary complex (ZMC)
Abstract
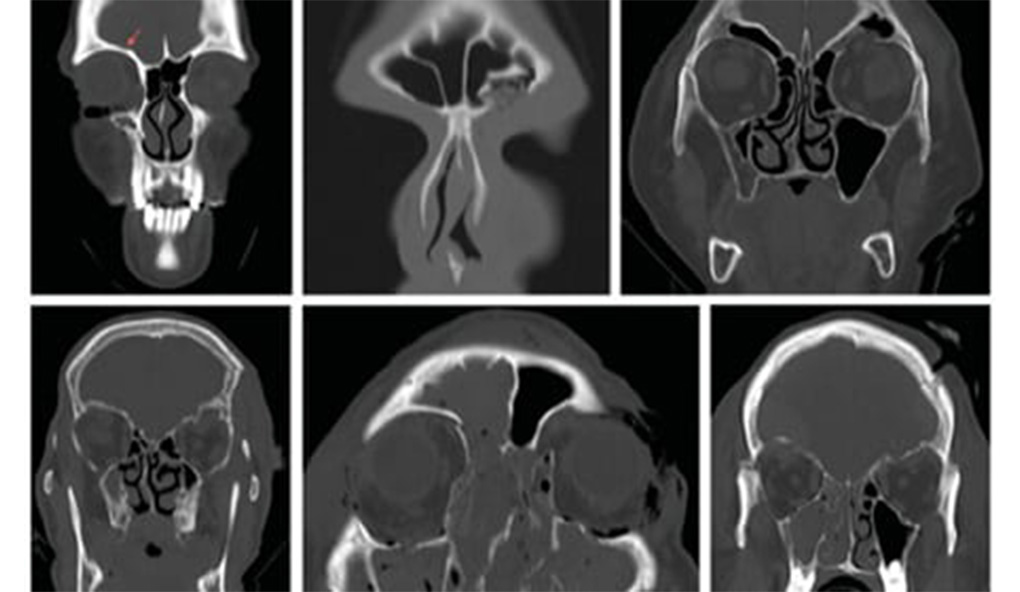
Orbital roof fractures are relatively uncommon in craniofacial surgery but present a management challenge due to their anatomy and potential associated injuries. Currently, neither a classification system nor treatment algorithm exists for orbital roof fractures, which this article aims to provide. This article provides a literature review and clinical experience of a tertiary trauma center in Australia. All cases admitted to the Royal Melbourne Hospital with orbital roof fractures between January 2011 and July 2013 were reviewed regarding patient characteristics, mechanism, imaging (computed tomography), and management. Forty-seven patients with orbital roof fractures were treated. Three of these were isolated cases. Forty were male and seven were female. Assault (14) and falls (13) were the most common causes of injury. Forty- two patients were treated conservatively and five had orbital roof repairs. On the basis of the literature and local experience, we propose a four-point system, with subcategories allowing for different fracture characteristics to impact management. Despite the infrequency of orbital roof fractures, their potential ophthalmological, neurological, and functional sequelae can carry a significant morbidity. As such, an algorithm for management of orbital roof fractures may help to ensure appropriate and successful management of these patients.